![]()
After receiving more and more interest on how an athlete’s heart responds to training we decided to ask one of Boston's experts on the subject. Amy Fiedler is a Cardiothoracic Surgery Fellow at The Massachusetts General Hospital in Boston, MA. She completed her undergraduate degree at Georgetown University in Washington DC where she studied Biology and ran Cross Country and Track. She then obtained a Master’s of Science in Microbiology and Immunology from Georgetown University prior to entering Medical School at The George Washington University. Following medical school, she began General Surgery Residency at The Massachusetts General Hospital, Harvard University and completed a two year research fellowship at The Brigham and Women’s Hospital, studying non-transplant surgical treatments for right ventricular failure. Her clinical interests include cardiovascular care of the athlete, cardiac adaptations to endurance sports, and surgical treatments of heart failure. Amy is an avid triathlete, two-time Ironman finisher, and is currently training for her third full Ironman, Ironman Mt. Tremblant in August of 2015.
Dr. Fiedler was asked six questions that range from the structure and function of a heart to the relationships of biomarkers and inflammation. Enjoy.
InsideTracker: Screening young athletes for risk of cardiac events is tricky because of the cost and expertise needed to analyze something as complex as the human heart. What is a good perspective for parents, athletes, and coaches involved with education on the subject matter?
Sudden cardiac death in a young athlete is a catastrophic event with enormous implications. These cases are of high public visibility given the unnerving nature of the death of a presumed healthy, young individual. As a result, screening young athletes in an attempt to prevent sudden cardiac death has become a hot topic issue.
It is important to recognize that sudden cardiac death, while devastating, is actually an infrequent event with an exceedingly low prevalence. In the athlete under the age of 35, the majority of sudden cardiac death is attributed to either congenital coronary artery anomalies or hypertrophic cardiomyopathy. When combined, authors note a combined 0.2% prevalence of these issues within the young athletic community.
What this means is that there is an exceptionally small number of athletes who will exhibit a congenital anomaly making them more likely to experience sudden cardiac death. As a result, screening each and every athlete for these rare occurrences is futile and not cost effective. I advocate for every athlete to see their primary care physician for a full history and physical examination prior to the start of each athletic season. A full cardiovascular personal and family history should be obtained at this visit, and if any abnormalities are encountered or clinical suspicion raised, further studies can be ordered.
![]()
These are both EKGs from athletes. Figure A demonstrates ST elevations, which are thought to be pathological in the correct population and indicative of a heart attack. However, in an athlete, this is actually the phenomenon of early repolarization, which is found in 50-80% of athletes and is idiopathic and benign. Figure B demonstrates a slight variation of the same phenomenon seen in Figure A.
InsideTracker: The endurance athlete's heart can make morphological adaptations (size and shape) that improve performance. What can team sports learn from these changes to improve their aerobic output? The research does point out untrained men do improve with adding recreational soccer to their fitness routine, but what about trained team sport athletes?
There is a constellation of cardiac morphological changes that have been described in the endurance athlete; we call them “The Athletes Heart.” Physiologic stressors as a result of performing endurance athletics for one or more hours most days cause the heart to adapt in accordance. When we exercise, we place increased volume and pressure demands on the heart as we ask it to pump harder and quicker in order to deliver oxygen to our working muscles. Over time, this increase in volume and pressure on the left ventricle causes the chamber to increase in muscle mass, wall thickness, and overall size. These adaptations are beneficial to the athlete, as a larger, more muscular left ventricle allows the heart to pump more volume at a higher pressure more efficiently.
Recent data in the medical literature cite advantageous morphological adaptation as demonstrated via echocardiography in a research study comparing two groups of hypertensive male subjects: group one made healthy life-style modifications by introducing a healthy diet without the addition of exercise. Group two ate a healthy diet and participated in six months of football training. While the hypertension improved in both groups, which is a beneficial clinical finding, cardiac structure was significantly modified in the football trained group, with improved cardiac function.
InsideTracker: Coaches and athletes have been using cold and hot temperatures to improve recovery. The research shows some conflicting summaries of the value of the concept. With regards to cardiac arrest, what is the current standing on the cooling and rewarming? Is it a safe bet that the heart is a great window to what is going on at the higher levels of the brain?
Cooling a patient who has experienced cardiac arrest has been a mainstay in treatment for many years after patients undergo CPR with return of spontaneous circulation. The patient is cooled as soon as possible for a total of 24 hours to a goal temperature of 32-34 degrees Celsius (89-93 F). Rewarming begins at hour 24 and is recommended at a rate no faster than 0.5 C per hour. For the most favorable outcomes, cooling must be done rapidly and instituted as early as possible. This is why pre-hospital CPR and return of spontaneous circulation following cardiac arrest is of utmost importance for the best results.
Yes, the heart can be viewed as a “window” of sorts into the brain. Cooling after cardiac arrest is done in order to protect the brain. The brain relies on oxygen and nutrient transport to its cells, which is pumped by the heart. When a patient experiences a cardiac arrest and the nutrient highway is halted to the brain, cerebral metabolism sharply declines, leading to rapid neurologic deterioration. The purpose of cooling is to slow the metabolic rate of the brain in order to minimize the damage.
InsideTracker: Heart Rate Variability (HRV) is growing with sports to monitor for fatigue, including the sport of Triathlon. Could you get into how the average person can understand the difference between morning pulse rate and something as sophisticated but now commercial like HRV?
Endurance athletes have long known that they have a lower resting heart rate when compared to more sedentary individuals. The reason for the low resting heart rate has to do with the hearts intrinsic adaptation, both electrically and structurally which results from the physiologic pressure and volume overload introduced while performing endurance activities. As a result, a low heart rate has long been associated with being in “good shape.” Heart Rate Variability (HRV) on the other hand, is a relatively new concept that specifically measures the time variation between individual heart beats. HRV was first utilized in the clinical setting as a prognostic indicator for mortality following myocardial infarction. HRV’s use has since expanded to the athletic scene as a relatively simple mechanism to track autonomic (sympathetic and parasympathetic) stimulation and therefore detect overtraining and poor recovery associated with sympathetic overdrive.
Research has demonstrated that athletes who are well recovered and trained have high HRV, while those that are experiencing stress and over-training have low HRV, independent of heart rate. This simple, non-invasive data point can be of significant utility to the majority of athletes who have a variety of stressors both in training and in life, as an early marker for a body that is over-stressed, under-rested, and over-trained.
InsideTracker: General wellness and heart health is not just about blood lipids anymore, inflammation and stress seem to be more researched in connecting biomarkers to heart health. What is a good take home message to the average weekend warrior or even elite athlete to creating balance for better recovery?
Absolutely correct. Heart health, while previously dictated as “healthy” based on levels of lipids, sugar, and cholesterol has increasingly shifted focus to the importance of inflammation and stress, most notably, the hormone cortisol. When the body is stressed, the fight or flight system (sympathetic nervous system) is activated. With activation of the sympathetic nervous system, our bodies release a series of hormones and chemicals in order to induce a heightened state of cardiovascular activity which is meant to be protective. Unfortunately, given the tremendous stress of daily living and responsibilities, most people these days have an overwhelming abundance of sympathetic stimulation. As with anything, too much of a good thing can turn ugly. The prolonged state of inflammation and sympathetic overdrive which is produced as a result of stress can be catastrophic to our bodies. Research has now implicated inflammation secondary to sympathetic stimulation as a main factor in the creation and progression of atherosclerosis, or hardening of the arteries, a significant risk factor for heart attacks in the adult population.
We can learn and extrapolate a lot with respect to lessons for the elite athlete or even the weekend warrior on how to best train and recover your heart and body from this interesting science regarding the sympathetic nervous system stimulation. For best performance, we all know that the body must rest and recover. More specifically, in the over-trained and under-rested/recovered athlete, stress hormones such as cortisol have been demonstrated to be increased, indicating an imbalance of sympathetic to parasympathetic innervation. What we can take away from this is the importance of training periodization, proper sleep and recovery time. While it may seem counterintuitive, your body tells you on a chemical and hormonal level when it is over-worked and tired. When this occurs, you are unable to reap benefits from your training, and instead place your body at risk of immune suppression and injury. The take home message is to sleep! Sometimes taking it easy is just as great for your training as a hard session.
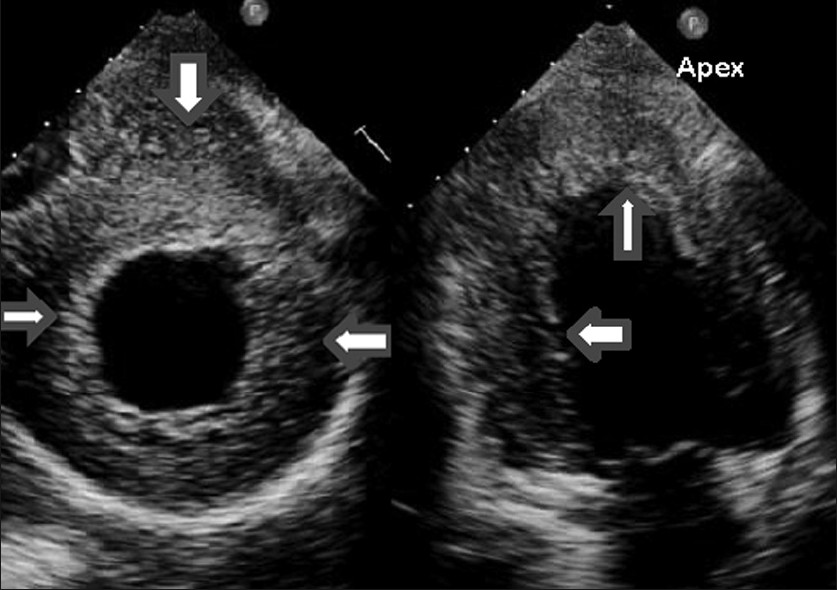
This is an echo image of a patient with left ventricular hypertrophy which is pathologic as a result of heart disease. You can appreciate how the wall thickness is similar to that seen in the endurance athletes heart
InsideTracker: Could you share a 30,000 foot view of what has disappointed you with sport science and cardiology today that you thought would be better by now? Finally, fast forward in five years what is the most exciting development you want to see in cardiology in sport?
Sport science and cardiology have come a long way. The field took off as a result of studying sudden cardiac death in athletes and has spiraled from there. Where we used to only have EKG and two dimensional echocardiography, we now have more sophisticated imaging tools, continuous monitoring devices, and the understanding and knowledge of the clinical importance of inflammatory and stress markers on cardiac physiology. That said, where we have made huge strides in studying the basic normal physiology of heart disease as it is a leading killer globally, the same push and strive for more information and accelerated creation of new technology has not been seen in the world of sports science. Much of what we still use and look at are the same values and tests that were used in the fields infancy. I think that we have the ability to delve far deeper into the workings, science, and manipulations of the athletes heart to more deeply understand the physiology and therefore push performance limits in the future.
Within the next five to ten years, I would be really excited to see real time, continuous three dimensional imaging of an athlete’s heart in action. Specifically, endurance athletes. I think that there is a lot to be learned from subtle wall motion changes and dynamic wall stress and tension physiology that we cannot fully appreciate when evaluating the heart at rest. I believe that this would be a powerful tool to further understand the “working mechanics” of an adapted heart.
We at InsideTracker wish to thank Dr. Fiedler for her time and expertise, and wish her well on her summer competitions in triathlon.
Note: Blogs on the InsideTracker website are for educational purposes only. Content shared are strictly for readers to be viewed as information, not a replacement for professional guidance from a healthcare professional.








