
Menopause is something that all women will inevitably go through, but few speak up about. Our philosophy is that when it comes to your health, every subject is open for discussion.
At InsideTracker, we’re not just here to throw biomarker stats at you and send you on your way; we want to help you understand the science behind them, and what your course of action should be once you do. And with such a wide array of symptoms, effects, related biomarkers, and potential remedies for menopause, it’s about time that someone started explaining. So we’re happy to step up.
What is menopause?
Menopause is classified by the absence of menstruation for 12 consecutive months, and onset usually begins for women in their 40s or 50s, with the average age of onset in the U.S. being 51. While menopause can be caused by things like a hysterectomy, cancer treatment, or medical conditions, it typically begins with ‘perimenopause’ in a woman’s 30s or 40s. During this time, menstrual cycles may become irregular or shorter in length, and are often accompanied by other symptoms.1
The association with middle age tends to be a major reason that people keep their menopausal status to themselves; many women mistake menopause as a sign of a weakening body. On the contrary! It’s the mark of a body that is functioning just as it should.
Why does menopause happen?
We’re born with all of the eggs our ovaries will ever have, and over the course of our menstruating lives, the cycling of hormones signals their release. As we age, our ovaries sense the emptying of our egg reserves. So, in response, they slow down the production of hormones like estrogen and testosterone to keep from wasting resources (their building blocks can be used elsewhere).
This decrease in sex hormones has far-reaching implications, from energy metabolism, to mood, and beyond. Perhaps most importantly, both play a role in the characteristic decline in bone mineral density (the best measurement of bone strength) that accompanies menopause. Estrogen is needed to replace weak and aging bone cells with young and resilient ones, while testosterone is classically responsible for anabolic processes (a.k.a. ones that build tissue rather than break it down) like bone formation.2

The benefits of menopause
This hormonal shift might seem to only have negative consequences, but it’s actually a testament to just how intuitive the human body is.
As we age, the likelihood of developing certain cancers increases. And some types, namely breast, ovarian, endometrial and colorectal, are estrogen dependent, meaning cancer cells harness the hormone for growth.3 So by reducing estrogen levels, your body is attempting to protect you from these diseases.
The loss of fertility is also a blessing in disguise; childbirth becomes riskier as we age. On average, women have achieved peak bone mineral density by 18 years old, which also happens to be when we’re most fertile.4 This is no coincidence, and low estrogen levels during menopause ensure suboptimally-dense bones won’t have to deal with the physiological stress of carrying a fetus’ weight.
For women who have traditionally struggled to maintain healthy iron levels, menopause has helped change that. With the lack of menstruation, daily iron needs decrease, and ferritin stores increase.
Menopause-related biomarkers
If you think you might be entering menopause or are wondering what biochemical changes occur during it, certain biomarkers can offer answers.
DHEAS: An estrogen precursor, DHEAS levels decline with age, further influencing estrogen’s downward trend along the menopausal transition.5
Testosterone: As we mentioned above, ovarian testosterone production decreases with age.5 Testosterone remains in circulation due to continued production by the adrenal glands.
SHBG: Sex Hormone Binding Globulin levels increase during menopause. SHBG binds estrogen and testosterone to reduce their effects (bound hormones are largely inactive) and increase the above-mentioned benefits of such inactivity. Low levels of SHBG are also associated with abnormal glucose and cholesterol metabolism as well as excess weight.6
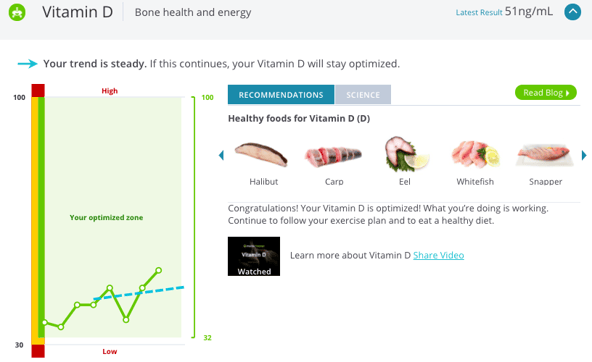
Vitamin D: Aging can cause a decrease in the formation of active vitamin D in our bodies, so your levels during menopause will reflect this. But vitamin D is incredibly important during the menopausal transition and beyond; it’s necessary for calcium absorption and the building of new bones.
Calcium: As one of the major structural components of bone, calcium’s importance during menopause cannot be overstated; sometime in her 30s, a woman’s body stops being able to produce new bone cells at the same rate at which they naturally degrade. This causes a decline in bone calcium content over time. Although serum calcium levels are tightly regulated and rarely indicate deficiency, this biomarker cannot go overlooked.
“Why are my symptoms different from hers?”
There’s a plethora of symptoms that come along for the menopausal ride. Some women (a lucky 5%) escape menopause without experiencing any, and 11% get hit “severely.”1 Chances are, you are, or will be, somewhere in the middle. But even then, your “moderate” won’t be the same as hers; while some menopausal symptoms are considered common, their combinations are often unique.
Hot Flashes
Hot flashes are the most common menopausal symptom, with about 75% of women experiencing them. They are often accompanied by cold sweats and facial flushing.1 Decreases in estrogen levels are widely considered to blame. After all, the centers in our nervous system that regulate body temperature are modulated by estrogen signals.1
While the connection might not feel obvious, hot flashes can also be to blame for sleeping irregularities. This can manifest as night sweats or general sleep disturbances.1,7
There are multiple documented treatments for alleviating hot flashes and their associated nighttime symptoms:
- Soybeans contain compounds called isoflavones which mimic estrogen in the body. Consuming whole soybeans or taking a daily 60 mg soy-based isoflavone supplement can help reduce the frequency and severity of hot flashes in peri- and postmenopausal women.8,9
- Studies showed that practicing mindful meditation when hot flashes occurred reduced accompanying distress and anxiety.10 If you’re new to meditation, try guided apps like Headspace.
- Studies show that weight loss is associated with decreased incidence of hot flashes and night sweats. If you’re rolling your eyes, we get it; it’s scientifically harder to lose weight as a postmenopausal woman than a premenopausal one. While there is no one tactic that works for everyone, good starting points may be to stay within your individual caloric needs, increase protein content (see below), and to exercise regularly.
- If you’re a smoker, you should know that by quitting, you can reduce the frequency and intensity of hot flashes, whether you’re currently experiencing them or will in the future. Even ex-smokers experienced worse vasomotor symptoms than those who never smoked. The earlier you quit, the better.
Depression and other mood disturbances
These are also common, affecting about a third of peri- and postmenopausal women.1 While depression is thought to be caused by decreases in estrogen and testosterone, there’s been recent debate over the safety of hormone therapy.11 Instead, certain lifestyle changes may prove useful in combating depressive symptoms:
- Studies have shown that women who engage in physical activity experience less mood and depressive symptoms than women who do not exercise.10,12
- Much like with hot flashes, mindfulness training can help to alleviate peri- and postmenopausal depressive symptoms.10,13
As a sex hormone, estrogen is also directly linked to vaginal function. Therefore other common symptoms include vaginal dryness, loss of vaginal elasticity, discomfort during sex, and reduced sex drive.14 At present, some OTC remedies may help to remedy these symptoms, but no lifestyle factors are known to help. Just know that if you’re experiencing them, you’re not alone.
Protect yourself from menopausal bone loss
Symptoms like the ones above are tangible and immediately relevant. But the accompanying, yet invisible bone loss, must be addressed just as vehemently. One in two women over the age of 50 will fracture a bone due to osteoporosis. Being on the right side of those odds means taking proactive and committed steps towards prevention.
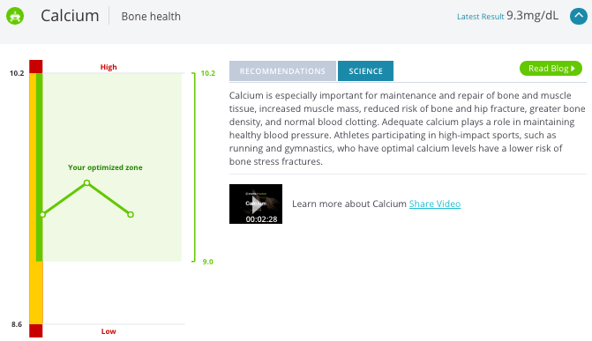
- Count your calcium. If you’re dairy free, your best options are fortified foods like non-dairy milk, juices, breads, and cereals. However, the best sources include dairy like yogurt and milk. Plant sources do contain calcium, but absorption issues render it null. Otherwise, take a 1,000 mg supplement daily, separate from meal time.
- Get plenty of vitamin D. It’s most plentiful in fatty fish and fortified dairy, but only roughly half of InsideTracker users have optimized vitamin D levels – your best bet might be to take a supplement. Get tested with InsideTracker to find out what’s right for you.
- Pay attention to protein. Studies show that people who ate greater than 0.8 g/kg protein per day tended to have higher bone mass.15,16
- Exercise! Do a mix of resistance (weight) training and impact-exercise like walking to build optimal bone mass.17,18
The female body is an incredibly complex system, and we know that keeping biomarkers, hormones, and recommendations straight can be difficult. So to take out the guesswork, we’ve sifted through the science to create our Female Reproductive Health goal. Whether you’re on hormonal birth control, trying to conceive, or at any stage of the menopausal process, our biomarker-specific recommendations can help you navigate the course.
References:
[1] Shanafelt, Tait D., et al. "Pathophysiology and treatment of hot flashes." Mayo Clinic Proceedings. Vol. 77. No. 11. Elsevier, 2002.
[2] Väänänen, H. Kalervo, and Pirkko L. Härkönen. "Estrogen and bone metabolism." Maturitas 23 (1996): S65-S69.
[3] “Estrogen and Cancer: Information & Risks.” Cleveland Clinic, 22 Aug. 2013.
[4] “Osteoporosis: Peak Bone Mass in Women.” National Institute of Arthritis and Musculoskeletal and Skin Diseases, U.S. Department of Health and Human Services, June 2015
[5] Burger, Henry G., et al. "Hormonal changes in the menopause transition." Recent progress in hormone research 57 (2002): 257-276.
[6] Overlie, Inger, et al. "The endocrine transition around menopause-a five years prospective study with profiles of gonadotropines, estrogens, androgens and SHBG among healthy women." Acta obstetricia et gynecologica Scandinavica 78.7 (1999): 642-647.
[7] Freedman, Robert R., and Timothy A. Roehrs. "Sleep disturbance in menopause." Menopause 14.5 (2007): 826-829.
[8] Cassidy, Aedin, Sheila Bingham, and K. D. Setchell. "Biological effects of a diet of soy protein rich in isoflavones on the menstrual cycle of premenopausal women." The American journal of clinical nutrition 60.3 (1994): 333-340.
[9] Mackey, R., A. Ekangaki, and J. A. Eden. "The effects of soy protein in women and men with elevated plasma lipids." Biofactors 12.1-4 (2000): 251-257.
[10] Lee, Youngwhee, and Hwasoon Kim. "Relationships between menopausal symptoms, depression, and exercise in middle-aged women: a cross-sectional survey." International journal of nursing studies 45.12 (2008): 1816-1822.
[11] Hui, Ling-yun, et al. "Association between MKP-1, BDNF, and gonadal hormones with depression on perimenopausal women." Journal of Women's Health 25.1 (2016): 71-77.
[12] Wang, Hui-Ling, et al. "Depressive symptoms in Taiwanese women during the peri-and post-menopause years: Associations with demographic, health, and psychosocial characteristics." Maturitas 75.4 (2013): 355-360.
[13] Green, Sheryl M., Brenda L. Key, and Randi E. McCabe. "Cognitive-behavioral, behavioral, and mindfulness-based therapies for menopausal depression: a review." Maturitas 80.1 (2015): 37-47.
[14] Shifren, JL, and S Hanfling. “Changes in Hormone Levels.” Changes in Hormone Levels, Sexual Side Effects of Menopause" | The North American Menopause Society, NAMS, Harvard University, 2010.
[15] Beasley, Jeannette M., et al. "Biomarker-calibrated protein intake and bone health in the Women's Health Initiative clinical ls and observational study." The American journal of clinical nutrition 99.4 (2014): 934-940.
[16] Remer, Thomas, Danika Krupp, and Lijie Shi. "Dietary protein's and dietary acid load's influence on bone health." Critical reviews in food science and nutrition 54.9 (2014): 1140-1150.
[17] Basat, Hande, Sina Esmaeilzadeh, and Nurten Eskiyurt. "The effects of strengthening and high-impact exercises on bone metabolism and quality of life in postmenopausal women: a randomized controlled trial." Journal of back and musculoskeletal rehabilitation 26.4 (2013): 427-435.
[18] Chien, M. Y., et al. "Efficacy of a 24-week aerobic exercise program for osteopenic postmenopausal women." Calcified tissue international 67.6 (2000): 443-448.








