 SHBG is a sex steroid binding protein that’s gotten a lot of bad rap in the past. But this may largely be based on faulty interpretation of in vitro research experiments that were not set up to answer an inherently physiologically complex question. In this blog we dig a little deeper and review some emerging findings on what SHBG is truly capable of, as well as give you some tips on how to use this biomarker to track your own metabolic health.
SHBG is a sex steroid binding protein that’s gotten a lot of bad rap in the past. But this may largely be based on faulty interpretation of in vitro research experiments that were not set up to answer an inherently physiologically complex question. In this blog we dig a little deeper and review some emerging findings on what SHBG is truly capable of, as well as give you some tips on how to use this biomarker to track your own metabolic health.

So….what’s new with SHBG?
Sex Hormone Binding Globulin, or SHBG, was discovered back in the 1960s for its ability to bind the hormones estradiol and testosterone. We’ve done quite a bit of work toward understanding more about this “carrier” protein, but have learned surprisingly little in the way of its multiple functions.
A large majority of doctors still have a unilateral view of SHBG as a biomarker that ties up sex hormones from binding their cellular receptors and thus prevents testosterone and estradiol from initiating downstream effects, such as bone remodeling and protein synthesis.
This may be because the protein’s multiple functions are far from thoroughly understood, but one thing is clear -- it’s anything but a simple carrier of sex steroids whose levels need to be minimized at all cost. In this blog, we’ll look at some very interesting findings that should make you (and your doctor) rethink how the SHBG lab test should (or should not) be interpreted.
The protein, the myths, and “new” science
The SHBG protein, along with albumin, are the primary plasma proteins responsible for binding testosterone and estradiol, with just 2-3% of the steroids believed to be free and unbound. SHBG is glycosylated, which means that it has sugar structures attached to it, and this, as we’ll see, can mean that the protein can vary in its characteristics from person to person depending on the genetic make-up.
For those who are scientifically inclined, or care to know, the average SHBG association constant for testosterone is approximately 1 x 109 L/mol, compared to albumin’s 3 x 104 L/mol. The larger number means that SHBG binds its ligand (testosterone) several-fold tighter than albumin. Its affinity for dihydrotestoterone, or DHT, is higher still. To add its fondness of sex steroids, SHBG also holds onto its ligands a lot longer than albumin -- up to 20 times!
All of this contributed to the hypothesis that it is only the free and albumin-bound steroids that are available to go to town within tissues. But, as we’ll see, this “guesstimate” was largely based on the limited information available at the time, and indeed, served as a simple model for MD’s to use when interpreting their patients’ lab results. But as we’ll see, though all of its functions do still remain elusive, SHBG research does reveal a few new tricks up the protein’s sleeve that largely debunk the free hormone hypothesis myth.
But before we go into how SHBG can deliver its cargo to cells, let’s look some more into how the protein’s properties can vary among individuals.
The free hormone hypothesis
According to the “free hormone hypothesis” only free steroids are biologically active, whereas those complexed with SHBG are inactive. As we’ll see, this notion can no longer be taken at face value.
First, the idea behind the hypothesis was that only the free or albumin-bound fractions could diffuse out of and capillaries and into cells. But, this was largely based on in vitro 1980s research in cultured cells. Here, the researchers found that testosterone could not get into these cells when SHBG was also present in the solution.
This kind of experimental set-up may be useful for looking at steroid-signaling pathways but it will tell you very little about whether SHBG will block any steroid in vivo! You see, academic researchers tend to pick cell types based on a what’s available, relatively easy to work with (some cell lines are NOT!), and not prohibitively expensive. That they chose a cell line without the capacity to interact with SHBG was unfortunate because it helped engrain the misleading notion that SHBG blocks testosterone from entering cells in general!
Had these experiments been performed using cells from sex steroid responsive tissues, such as prostate or endometrium, the results would have been very different!
The lesson is that there is no way to represent all the different cell types and their myriad of differentially expressed receptors that are present in our bodies, so we should be very careful when extrapolating the results of isolated experiments to our higher-level physiology!
With this out of the way, let’s now look at a couple of known partners that SHBG likes to interact with...
SHBG receptor
That intracellular SHBG exists was described over four decades ago, and it is now clear that there is a SHBG-specific cell surface receptor (termed RSHBG) that binds the molecule in its free form (but not bound to T or E2). The SHBG-receptor complex is activated (or inhibited) by certain steroids (SHBG can bind steroids with affinity equal to its solution state once bound to RSHBG) and signals a chain of events that begin with generation of cyclic adenosine monophosphate (cAMP), with the downstream effects being tissue dependent.
The fact that SHBG’s downstream intracellular effects involve cAMP is an exciting finding in and of itself because this second messenger is a key player in relaying messages from hormones on the outside to the inside of the cells. cAMP is also involved in turning on enzymes (called protein kinases) that regulate the effects of molecules like adrenaline and glucagon. The exact mechanism of how the binding and activation of the SHBG-RSHBG complex affects cells is still unclear, but judging from the clinical metabolic trends and correlations we see (described below) these effects are definitely real.
Interestingly, RSHBG’s actions are independent of the androgen and estrogen receptors, and it seems like location is key because the same steroid can either inhibit or activate the receptor depending on the tissue type.
So, as you see, SHBG is not the evil annihilator of sex steroid action, but may actually have a role in enhancing it in a tissue-specific manner. But there is more...
Megalin
Megalin, a member of the LDL protein family, is another cell-surface receptor known to be a key player in Vitamin A & D metabolism. These vitamin hormones also tend to be bound by plasma proteins and, when they encounter megalin, this receptor is able to sequester them into the intracellular environment.
Once within the cell, the carrier proteins are degraded and the ligands (in this case, Vitamins A & D) are released into the cytosol for further metabolism. Recent work indicates that megalin is also expressed in sex-steroid responsive tissues (including skeletal muscle!) and similarly internalizes SHBG-bound steroids! More research is needed into the true significance of this finding, but it certainly adds to mounting evidence that SHBG may be an active little protein in all things metabolism.
Furthermore, there is some evidence that SHBG itself can also be synthesized in tissues other than the liver, creating the possibility of local modulation effects of on steroid hormone action.
Bottom line
Taken together, the body of research on SHBG’s multiple functions puts the biomarker’s level fluctuations into context. That Joe has a SHBG level of 50 nmol/L level and Jeff has 30 nmol/L and both have the same plasma testosterone concentration (in the optimal range) does not necessarily mean that Jeff is better off due his higher free testosterone. That’s because tissue distribution of both RSHBG, megalin, as well as the presence of SHBG glycosylation variants all factor into the ability of testosterone to enter various responsive tissues and the plasma clearance of the steroid.
Thus, SHBG is a multifunctional player that can orchestrate steroid action to a degree far greater than that attributed to it just through its binding ability, so I think it’s safe say that the free hormone hypothesis is a myth, at least in its absolute sense.
With the protein biochemistry out of the way, we now have better context to understand what could be behind the SHBG lab test’s already established utility and the trends we see in actual people.
The Blood Test
The SHBG blood test itself was developed in the early 1970’s and has since been used to assess various conditions related to the metabolism of androgens and estrogens, both of which primarily circulate in the protein-bound form. Conditions where SHBG levels are clinically relevant include various diseases requiring sex steroid therapy, diagnosis of puberty and thyroid disorders, and anorexia nervosa. In addition, while it is not yet a common clinical practice to use SHBG as a biomarker for metabolic syndrome, a plethora studies indicate the protein’s significant utility in this realm as well.
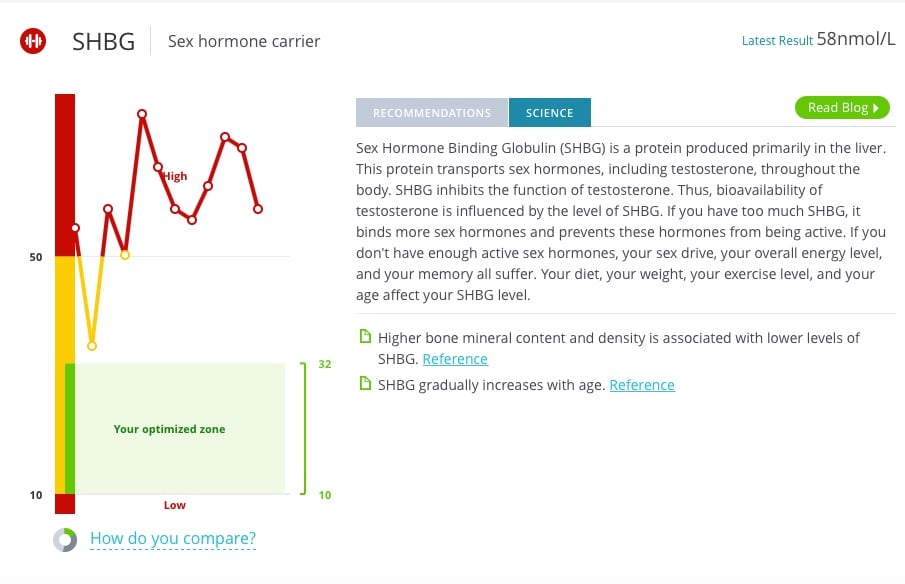
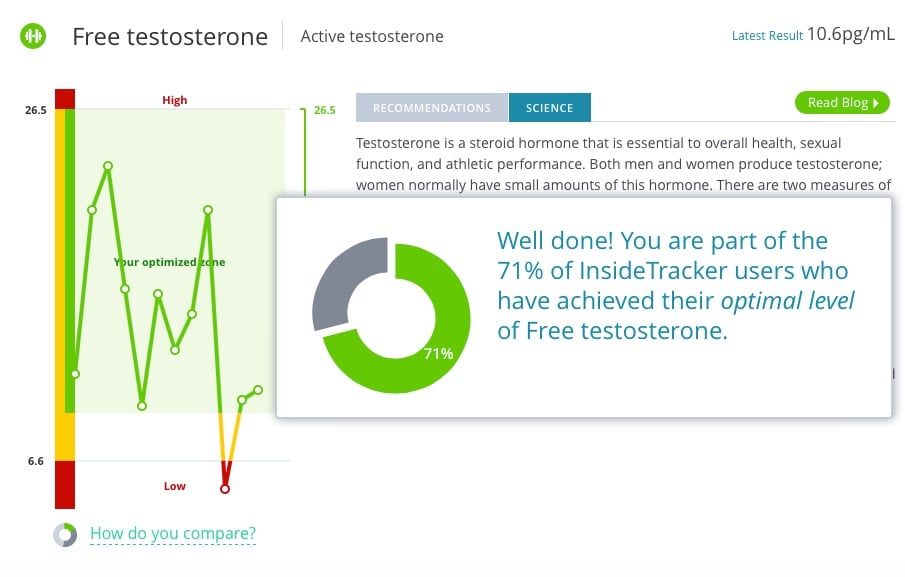
In fact, in the context of striving to optimize your health with InsideTracker, the SHBG test can be a useful tool to track how you’re doing metabolically.
Key findings: Trends we see in real people
Scientific literature describes a now well-established negative correlation between obesity, type 2 diabetes, cardiovascular disease and SHBG. In other words, those with the Metabolic Syndrome are known to have low plasma levels of the protein.
More recently, however, the most important factor that was teased out of this correlation was liver fat, not BMI itself. So, if you’re genetically predisposed to depositing fat in the liver it is possible to have low SHBG while being relatively lean. This genetic predisposition was studied, with some interesting results.
Ethnicity Matters
African Americans seem to be protected from fatty liver, or steatosis, as only 24% get it on average, while those of Hispanic origins exhibit higher frequencies (close to 50%). European Americans fall in the middle, with around a third of the population showing predisposition to hepatic fat.
These observations also correlate well with basal SHBG levels. Importantly, low SHBG levels also showed a significant relationship with the release of liver enzymes and increased hepatic inflammation. This inflammation association was limited to those of Hispanic origins -- the group with the greatest prevalence of fatty liver, lowest SHBG, and susceptibility to cirrhosis.
It’s also worth mentioning that total body fat and visceral fat do not correlate well with SHBG levels, again questioning the original assumption that a high BMI meant low SHBG.
So, in essence, these studies in people show that basal SHBG levels are largely genetically determined and, when we allow them to go too low, it can mean that we may be heading in the wrong direction, metabolically speaking.
In fact these intriguing findings point to SHBG as a potential biomarker for both Metabolic Syndrome and the associated inflammation (we will cover the “how” below).
Indeed, the research community has coined a new term -- metaflammation -- to describe a low-grade, obesity-driven inflammatory state that’s been shown to separate the “healthy” obese from the “unhealthy” ones. Could SHBG be a relevant biomarker as part of a toolkit to assess metaflammation in the future? Based on the protein’s intimate involvement in modulating sex steroid action and clearance rates, its predictive value in steatosis, as well as the regulatory mechanisms I’ll describe below, it appears that it just may be a logical candidate!
Dynamics of SHBG regulation: understanding what’s behind a number
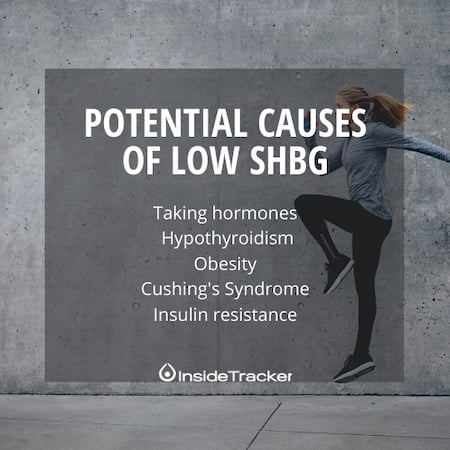
So far, I think the message is clear that low SHBG levels are indicative of suboptimal metabolic status, but are you doomed if your levels are below a certain level? Not necessarily. You see, as long as you know your genetic healthy baseline and you arm yourself with what external factors can affect that baseline, you have the tools to understand fluctuations in your SHBG, and be able to adjust your diet and/or lifestyle accordingly should you see an unexpected result. Now let’s go into some well-established, as well as some new and exciting, factors that are known to significantly affect the levels of this biomarker.
Androgens and Estrogens
Potent androgens like testosterone reduce SHBG production in the liver. On the other hand, estrogen-simulating drugs like birth control pills or selective estrogen receptor modulators (SERMs) tend to increase SHBG production. The former is well documented because women’s use of oral contraceptives is associated with increased sexual health complaints, in part by decreased androgen production and in part through skyrocketing SHBG levels.
Fortunately, emerging research has now caught up with some of these once purely empirical/clinical observations, with the proposed mechanism involving the adipose tissue-secreted adipokine hormone, called adiponectin. What researchers found was that adiponectin stimulates a pathway, known as the AMPK pathway, which leads to increased production of SHBG through the HNF4-4A protein and reduction in hepatic triglyceride levels. This makes perfect sense, because, as I mentioned above low SHBG is associated with fatty liver disease and Metabolic Syndrome and those with the syndrome also have low adiponectin levels!
You may ask, so what does testosterone have to do with it? And will taking estrogenic compounds improve my metabolism since it drives SHBG up?
Well, testosterone has now been shown to reduce adiponectin levels, which explains why testosterone tends to reduce SHBG levels. This finding also explains why women, who have lower androgen levels and thus higher average adiponectin levels, show higher levels of SHBG.
We should keep this dynamic picture of SHBG regulation in context, however. As long as we are talking about endogenous testosterone and estrogen, then the associated SHBG fluctuation should be in the healthy range (provided no underlying illness). However, those prescribed steroids and women on oral contraceptives should carefully monitor their SHBG level as these exogenous steroids can lead to excessive spikes or reductions in this biomarker.
Insulin
The effects (or lack thereof) insulin are worth mentioning because it was once thought that this powerful hormone decreased SHBG production in the liver. However, this finding has now been debunked by more recent interpretation of the data. It was found that insulin’s effects were not specific to SHBG and the reduction in hepatic protein secretion was more global (i.e. nonspecific). Moreover, this finding was observed in transformed (cancerous) cells which may not reflect the biology of normal liver cells, particularly since in vivo models have not reproduced this trend, and to the contrary have shown that insulin may increase SHBG, probably due to its inhibitory effects on proinflammatory cytokines.
Cytokines
SHBG has been shown to be downregulated by a couple of inflammation-inducing cytokines known as TNFɑ and IL-1β. That inflammation reduces SHBG levels is also evidenced by the trend for low grade inflammatory diseases such as obesity, diabetes, osteoarthritis, etc. to result in patients with lower SHBG levels.
It is interesting to note that these inflammatory diseases are also associated with low testosterone. We now know that this could result from the combined effects of low grade inflammation and reduced adiponectin levels, both of which would downregulate SHBG production at the liver and result in elevated clearance rate of testosterone from blood, thus resulting in a low plasma testosterone blood test result.
These findings, again, point to SHBG as being a great candidate as a biomarker for metaflammation.
Diet
Studies on the effects of dietary protein on SHBG levels have yielded inconclusive results, and, provided sufficient surplus of the macronutrient, any observed increases in SHBG levels may be due to overall increase in protein synthesis.
But, it has been shown that high carbohydrate - and in particular, fructose - diets induce de novo lipogenesis and accumulation of liver fat, which as described above has the effects of decreasing SHBG though the HNF-4A pathway. This finding is consistent with the concept that insulin is not significantly involved in SHBG regulation since fructose does not stimulate insulin secretion from the pancreas.
Clinical data also reveals that olive oil consumption is associated with elevated SHBG serum levels, a finding that is in agreement with the low incidence of metabolic disease and improved longevity in the Mediterranean population. This finding is also supported by data showing that oleate intake upregulates SHBG production via downregulation of the peroxisome proliferator-activated receptor gamma (PPARɣ), a key regulator of metabolism from the PPAR family of transcription factors.
Exercise
Both intense resistance and endurance type exercise increase SHBG production. Interestingly, in resistance exercise, despite potentially decreasing free testosterone levels, SHBG correlates with increased hypertrophy and muscle strength, though now that we know that specific SHBG receptors do exist (i.e. RSHBG and megalin), this result is not as surprising.
On the other hand, in endurance training, excessive training can result in a HPGA suppression and thus a drop in both total and free testosterone more quickly, sometimes leading to compromised sexual health.
In essence, balance is key! Both resistance and endurance activities have a place, but it’s important not to overdo either. If your SHBG level is rising significantly, you may want to reevaluate the intensity and/or volume of your exercise regimen, or simply implement more recovery time.
Making the science work for you
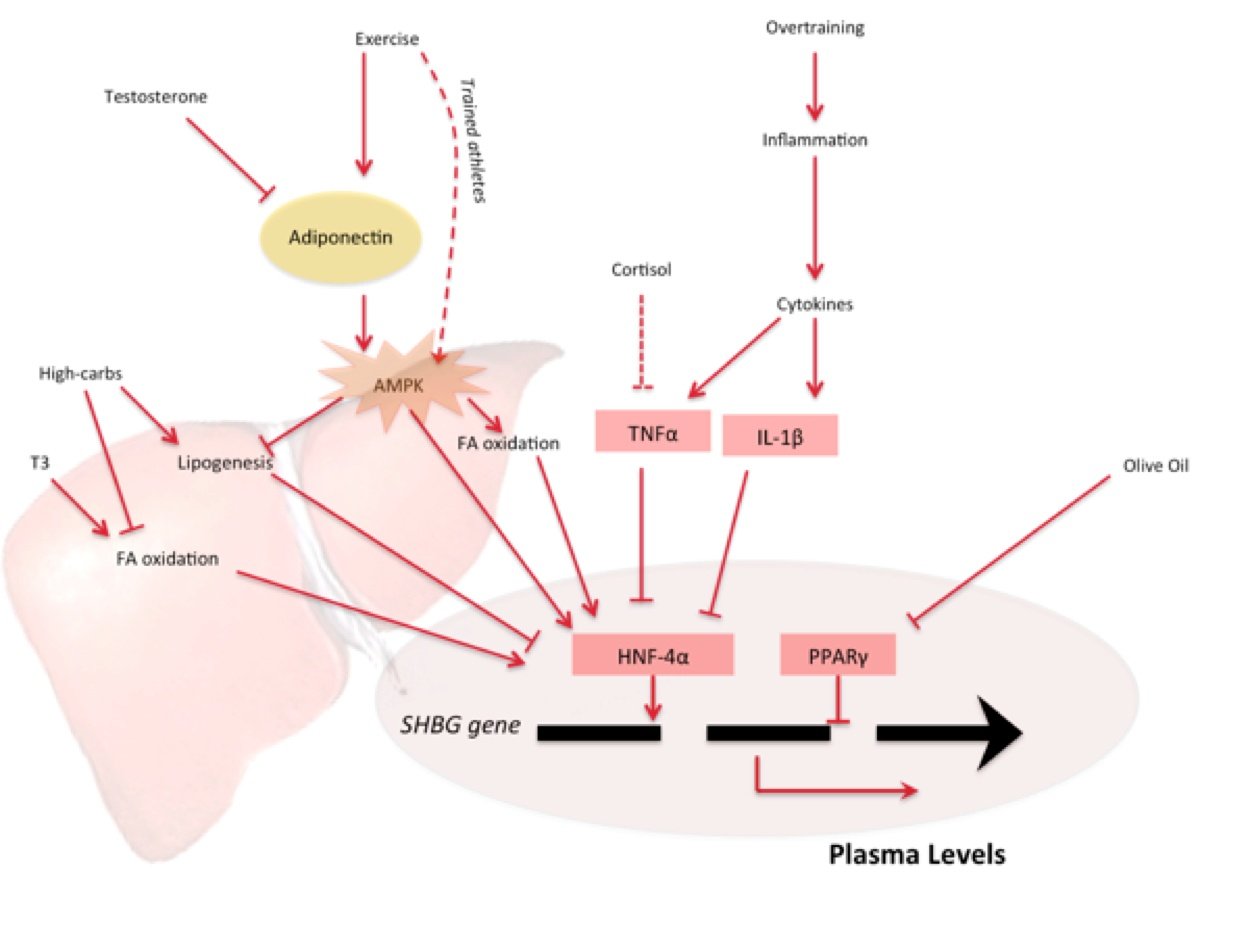
In order to use SHBG as a biomarker as an additional tool to see where you stand on your quest to optimize your metabolism it is important to establish a reliable baseline first. This can mean more than a single blood draw when there are no underlying illnesses, your workout regimen is reasonable, and your diet on track. In particular, you want to make sure you are not overtraining or eating excess fructose (not to mention avoiding high-fructose corn syrup!). With this established, you can track your progress by assessing your SHBG levels as part of a larger picture using our multiple other biomarkers. The graphic below summarizes some of the points I covered in this blog:
If you find that your baseline is very high in the normal range, or just outside of it, it might be a good idea to evaluate your exercise regimen. For example, if you run marathons or otherwise engage in lots of endurance activities (or other forms of strenuous exercise) you may find that reducing the volume for a few weeks to months may help balance out your SHBG. Conversely, if you find that your SHBG is unexpectedly low, you can look to your diet to ensure you’re not over-consuming carbohydrates or otherwise causing a lifestyle-induced inflammatory state (such as being too sedentary) that’s driving this biomarker down. In this case, you may want to reduce your carbs, add more olive oil to your diet and/or increase your activity levels to bring your SHBG levels up.
Whatever you do, don’t freak out if you see this biomarker on the rise but still in the healthy range, as we now know that SHBG’s cargo is still being delivered to where it’s meant to be.
References:
Coviello, A. D., Haring, R., Wellons, M., Vaidya, D., Lehtimäki, T., Keildson, S., … Perry, J. R. B. (2012). A genome-wide association meta-analysis of circulating sex hormone-binding globulin reveals multiple loci implicated in sex steroid hormone regulation. PLoS Genetics, 8(7). doi:10.1371/journal.pgen.1002805
De Ronde, W., Van Der Schouw, Y. T., Muller, M., Grobbee, D. E., Gooren, L. J. G., Pols, H. a P., & De Jong, F. H. (2005). Associations of Sex-Hormone-Binding Globulin (SHBG) with Non-SHBG-Bound levels of testosterone and estradiol in independently living men. Journal of Clinical Endocrinology and Metabolism, 90(1), 157–162. doi:10.1210/jc.2004-0422
Hammes, A., Andreassen, T. K., Spoelgen, R., Raila, J., Hubner, N., Schulz, H., … Willnow, T. E. (2005). Role of endocytosis in cellular uptake of sex steroids. Cell, 122(5), 751–762. doi:10.1016/j.cell.2005.06.032
Jürimäe, J., Mäestu, J., Jürimäe, T., Mangus, B., & Von Duvillard, S. P. (2011). Peripheral signals of energy homeostasis as possible markers of training stress in athletes: A review. Metabolism: Clinical and Experimental, 60(3), 335–350. doi:10.1016/j.metabol.2010.02.009
Kahn, S. M., Hryb, D. J., Nakhla, a M., Romas, N. a, & Rosner, W. (2002). Sex hormone-binding globulin is synthesized in target cells. The Journal of Endocrinology, 175(1), 113–120.
Lira, F. S., Rosa, J. C., Pimentel, G. D., Tarini, V. a F., Arida, R. M., Faloppa, F., … Santos, R. V. T. (2010). Inflammation and adipose tissue: effects of progressive load training in rats. Lipids in Health and Disease, 9, 109. doi:10.1186/1476-511X-9-109
Margonis, K., Fatouros, I. G., Jamurtas, A. Z., Nikolaidis, M. G., Douroudos, I., Chatzinikolaou, A., … Kouretas, D. (2007). Oxidative stress biomarkers responses to physical overtraining: Implications for diagnosis. Free Radical Biology and Medicine, 43(6), 901–910. doi:10.1016/j.freeradbiomed.2007.05.022
Marin, D. P., Bolin, A. P., Campoio, T. R., Guerra, B. A., & Otton, R. (2013). Oxidative stress and antioxidant status response of handball athletes: Implications for sport training monitoring. International Immunopharmacology, 17(2), 462–470. doi:10.1016/j.intimp.2013.07.009
Maynar, M., Timon, R., González, A., Olcina, G., Toribio, F., Maynar, J. I., & Caballero, M. J. (2010). SHBG, plasma, and urinary androgens in weight lifters after a strength training. Journal of Physiology and Biochemistry, 66(2), 137–142. doi:10.1007/s13105-010-0018-6
Nakhla, a. (1999). Sex hormone-binding globulin receptor signal transduction proceeds via a G protein. Steroids, 64(3), 213–216. doi:10.1016/S0039-128X(98)00084-1
Ng, K. M., Catalano, M. G., Pinós, T., Selva, D. M., Avvakumov, G. V., Munell, F., & Hammond, G. L. (2006). Evidence that fibulin family members contribute to the steroid-dependent extravascular sequestration of sex hormone-binding globulin. Journal of Biological Chemistry. doi:10.1074/jbc.M512370200
Pugeat, M., Moulin, P., Cousin, P., Fimbel, S., Nicolas, M. H., Crave, J. C., & Lejeune, H. (1995). Interrelations between sex hormone-binding globulin (SHBG), plasma lipoproteins and cardiovascular risk. The Journal of Steroid Biochemistry and Molecular Biology, 53(1-6), 567–572. doi:10.1016/0960-0760(95)00102-6
Pugeat, M., Nader, N., Hogeveen, K., Raverot, G., Déchaud, H., & Grenot, C. (2010). Sex hormone-binding globulin gene expression in the liver: Drugs and the metabolic syndrome. Molecular and Cellular Endocrinology, 316(1), 53–59. doi:10.1016/j.mce.2009.09.020
Rosner, W. (2006a). Sex steroids and the free hormone hypothesis [1]. Cell, 124(3), 455–456. doi:10.1016/j.cell.2006.01.026
Rosner, W. (2015). Free estradiol and sex hormone-binding globulin. Steroids, 99, 113–116. doi:10.1016/j.steroids.2014.08.005
Rosner, W., Hryb, D. J., Kahn, S. M., Nakhla, A. M., & Romas, N. a. (2010). Interactions of sex hormone-binding globulin with target cells. Molecular and Cellular Endocrinology, 316(1), 79–85. doi:10.1016/j.mce.2009.08.009
Rosner, W., Hryb, D. J., Khan, M. S., Nakhla, a M., & Romas, N. a. (1999). Sex hormone-binding globulin mediates steroid hormone signal transduction at the plasma membrane. The Journal of Steroid Biochemistry and Molecular Biology, 69, 481–5. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/10419028
Sáez-López, C., Soriguer, F., Hernandez, C., Rojo-Martinez, G., Rubio-Martín, E., Simó, R., & Selva, D. M. (2014a). Oleic acid increases hepatic sex hormone binding globulin production in men. Molecular Nutrition & Food Research, 58(4), 760–767. doi:10.1002/mnfr.201300304
Shea, J. L., Wong, P.-Y., & Chen, Y. (2014). Free Testosterone. Advances in Clinical Chemistry (1st ed., Vol. 63). Elsevier Inc. doi:10.1016/B978-0-12-800094-6.00002-9
Simó, R., Sáez-López, C., Barbosa-Desongles, A., Hernández, C., & Selva, D. M. (2015). Novel insights in SHBG regulation and clinical implications. Trends in Endocrinology & Metabolism, 1–8. doi:10.1016/j.tem.2015.05.001
Simó, R., Saez-Lopez, C., Lecube, A., Hernandez, C., Fort, J. M., & Selva, D. M. (2014). Adiponectin upregulates SHBG production: Molecular mechanisms and potential implications. Endocrinology, 155(8), 2820–2830. doi:10.1210/en.2014-1072
Smith, L. L. (2000). Cytokine hypothesis of overtraining: a physiological adaptation to excessive stress? Medicine and Science in Sports and Exercise, 32(2), 317–331. doi:10.1097/00005768-200002000-00011
Steinacker, J. M., Lormes, W., Reissnecker, S., & Liu, Y. (2004). New aspects of the hormone and cytokine response to training. European Journal of Applied Physiology, 91(4), 382–391. doi:10.1007/s00421-003-0960-x
Vandenput, L., & Ohlsson, C. (2014). Genome-wide association studies on serum sex steroid levels. Molecular and Cellular Endocrinology, 382(1), 758–766. doi:10.1016/j.mce.2013.03.009
Wedick, N. M., Mantzoros, C. S., Ding, E. L., Brennan, A. M., Rosner, B., Rimm, E. B., … van Dam, R. M. (2012). The effects of caffeinated and decaffeinated coffee on sex hormone-binding globulin and endogenous sex hormone levels: a randomized controlled trial. Nutrition Journal, 11(1), 86. doi:10.1186/1475-2891-11-86
Wu, T.-S., & Hammond, G. L. (2014). Naturally occurring mutants inform SHBG structure and function. Molecular Endocrinology, 28(7), 1026–1038. doi:10.1210/me.2014-1058








