
Fitness Dogma says weightlifting makes you stronger and larger, which is good for men and bad for women. New research says that regular resistance training can do much more than make men more muscular: it can boost heart health and fight aging in both men and women. Additionally, a recent study indicates that there are unique biomarker benefits to sticking with that regular weightlifting program long after you get start a program. Below we examine why you want to adopt a weightlifting program- and stick with it.
Weightlifting and Anti-Aging
Strength training, also known as resistance training, is a type of physical exercise that uses resistance to contract skeletal muscles such as biceps, triceps, and quadriceps. Its main purpose is to build strength, increase the size of muscles, and improve anaerobic endurance (i.e. quick, powerful exercises such as sprinting). The most common forms of strength training exercises are weight-bearing movements that use dumbells or barbells, such as bench press and deadlifts, or bodyweight such as pull-ups and push-ups. Other forms of strength training include plyometrics, kettlebells, and powerlifting
Historically and culturally, resistance training is associated with increasing strength in athletes and physical attractiveness in men. However, many studies conducted in both men and women of all ages have shown a variety of positive health effects resulting from regular resistance training. As a result of credible research, the American College of Sports Medicine has included strength training in its annual list of recommendations since 1998 for maintaining optimal cardiovascular health and overall wellness. 1

Why was this Study Done?
Despite rigorous research on strength-training, few research studies have assessed if these changes are influenced by prior experience with resistance training exercise. As a result, researchers designed a study published in the highly regarded AGE Journal in October of 2015 and sought to evaluate two main questions:
- What positive health effects are observed in people who start resistance training?
- What differences in strength, body composition, and biomarkers are noted in people who are committed strength-trainers versus those new to resistance training?
Before we look at the study’s interesting results, though, we need to examine how the study was designed.
Who was In the Study?
Sixty-five women at least 60 years in age were recruited for this study. They had an average age of 68.9 years and an average BMI of 27.6 kg/m2. 2 They were all relatively healthy, had normal blood pressure, and were non-smokers. Additionally, they were non-diabetic and had no cardiovascular (heart) or renal (kidney) dysfunction. However, none of them had participated in regular physical exercise for more than once per week in the six months prior to the intervention study.

Quick Summary: Researchers conducted this study on 65 healthy, women with no history of chronic conditions or regular physical exercise in the past six months.
The Weight Training Study Design
Scientists divided the 65 subjects into two groups. The first group of 35 subjects underwent three phases of weight training while the second group of 30 subjects participated in one phase of weight training. Because the first group has more extensive training than the second, they were labeled the “advanced group” while the second was named the “novice group.”
The study, which was 40 weeks in length, was divided into four 2-day rest phases and three training phases. During the rest phases, scientists measured key metrics related to fitness including body composition, one repetition maximum, and biomarkers such as triglycerides, glucose, and LDL-cholesterol. The three training phases were as follows:
Training Phase 1 (Weeks 3-14)
- The advanced group participated in weightlifting exercises 3 times per week (Monday, Wednesday, Fridays) for 12 weeks
- The novice group did not participate in this phase
- The exercise regimen consisted of 8 resistance exercises performed for 10-15 repetitions for one set each
- Between each exercise, the subjects rested 2 to 3 minutes
- The exercises in each regimen covered the entire body and included leg curls, bench press, and seated row
Training Phase 2 (Weeks 17-28)
- The advanced group underwent another 12-week period where they participated in 8 different weightlifting exercises 3 times per week
- The novice group again did not participate
- The exercise regimen consisted of 8 resistance exercises performed for 10-15 repetitions for two sets each this time
- Between each set for the same exercise, the subjects rested 1 to 2 minutes
- Between two different exercises, subjects rested 2 to 3 minutes
Training Phase 3 (Weeks 31-38)
- For eight weeks, both the novice and advanced group participated in an eight-week training session
- The exercise regimen consisted of 8-12 repetitions for three sets this time
- Between each set for the same exercise, the subjects rested 1 to 2 minutes
- Between two different exercises, subjects rested 2 to 3 minutes
Throughout the trials, the subjects were asked to maintain their typical dietary consumption. During rest periods, scientists assessed key data related to health, recovery, and fitness performance.
Quick Summary: The women were divided into two groups. The first one participated in regular weightlifting for 24 weeks and were known as the advanced group. Then, the advanced group and a group of untrained females (called the novice group) participated in an eight-week resistance training program.
What Was Measured?
Researchers assessed metrics of body composition metrics before the study, during the rest periods, and at the conclusion of the study. When comparing the two groups, they looked at the advanced and novice groups before and after the 8-week phase. They specifically examined:
- Body fat Percentage
- One-rep max Chest press (kg)
- One-rep max Knee extension (kg)
- One-rep max Preacher curl (kg)
- Total strength (kg), the sum of the three one-rep maxes
- Skeletal muscle mass (kg)
Additionally, they looked at the six following biomarkers critical to health and performance. One of them, called C-reactive protein (CRP), is a critical components of InsideTracker’s InnerAge panel. The other five are part of the metabolic panel in InsideTracker’s Ultimate test. Below are the biomarkers in a bit more detail:
C-Reactive Protein (CRP): CRP is a ring-shaped molecule consisting of five proteins. It is part of the immune system and released into the bloodstream a few hours after an inflammatory response resulting from infection by a foreign cell or tissue injury. Many studies show that consistently high levels of CRP are strongly associated with depression, many cardiovascular diseases, and diabetes. 3,4 Additionally, research indicates that rigorous exercise with insufficient recovery can lead to cell injury and increased CRP production. 5
Glucose (mg/dL): The body gets its energy from a sugar named glucose through a process called cellular respiration. Adequate levels of glucose are essential for the body’s proper function. However, high concentrations of blood glucose can slow down blood flow and lead to a variety of chronic complications such as type II diabetes and severe fatigue.
Triglycerides (mg/dL): Fat molecules in the blood called triglycerides store energy for later use. While they are essential for energy production, consistently elevated blood levels of triglycerides are associated with an increased risk of a variety of cardiovascular diseases and kidney complications. 6,7
Total cholesterol (mg/dL): Cholesterol is essential for properly functioning cell membranes, forming hormones, and facilitating the absorption of certain vitamins. 8,9 If we aren’t care with our diet, though, cholesterol can elevate to unhealthy levels and lead to similar complications. 9 Thus, it is crucial to use InsideTracker analysis to learn your cholesterol and the best interventions to utilize in order to optimize its levels.
HDL-C (mg/dL): High density lipoprotein (HDL) transports cholesterol around the body. Additionally, it collects brings excess cholesterol not being used by the body to the liver where it is recycle or destroyed. By doing this, HDL prevents cholesterol from accumulating in blood vessels and clogging them. Several studies showed an inverse association between cardiovascular disease and levels of HDL-C and there is a general consensus among clinicians that higher levels of HDL-C are good for the body. 10,11,12
LDL-C (mg/dL): Low-density lipoprotein, also known as LDL, is produced by the liver and cells throughout the body. Unlike HDL, LDL molecules move slowly in the bloodstream and are prone to oxidizing agents called free radicals. Once they are oxidized, LDL oftentimes burrows itself into walls of arteries and slows down blood flow. High concentrations of LDL-C are associated with a heightened risk of cardiovascular diseases including stroke and type II diabetes. 13 Clinical evidence indicates that decreasing levels of LDL-C can reduce your risk of developing cardiovascular diseases. 14,15
Summary: Researchers measured markers of strength and body composition in the subjects before and after the weightlifting intervention. They also assessed levels of six biomarkers measured by InsideTracker associated with health and fitness: C-reactive protein (CRP), triglycerides, HDL cholesterol (HDL-C), LDL cholesterol (LDL-C), and glucose.
Results of the Study
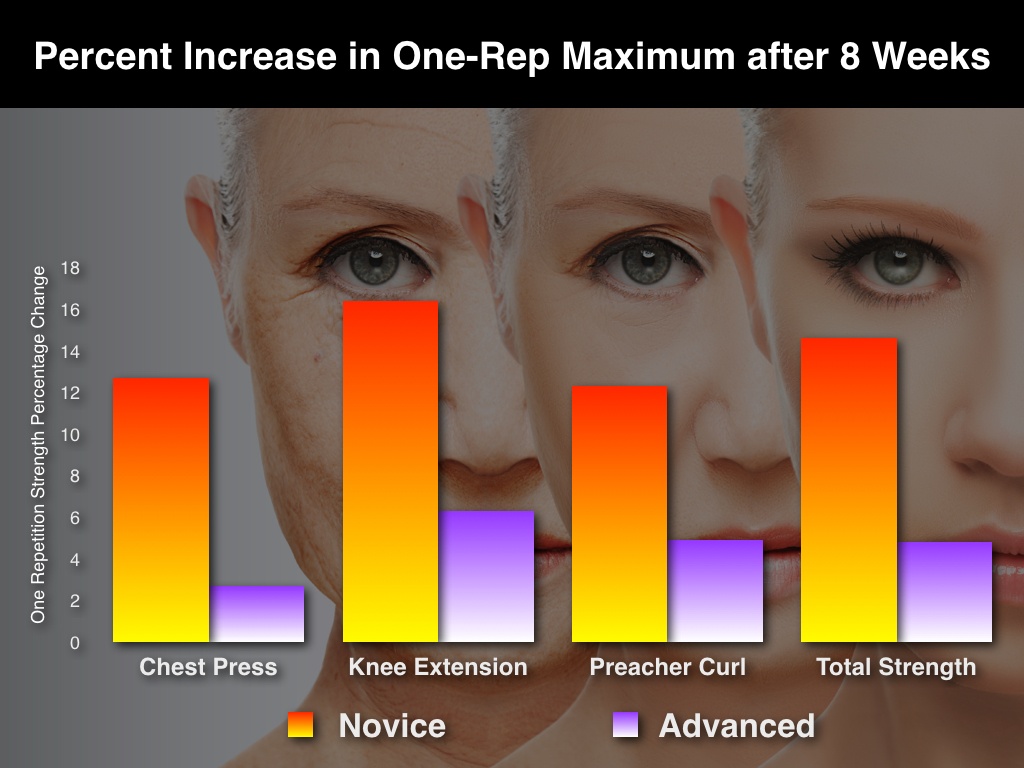
As expected, the subjects in the novice group experienced more pronounced changes in all metrics related to fitness during the third, eight-week long training phase. More specifically, average one-rep max chest press increased by 12.7% from 35.5kg to 40.0 kg, average one-rep max knee extension increased 16.4% from 39.0 kg to 45.4 kg, and average one-rep max preacher curl increased 12.3% from 19.5kg to 21.9 kg. 2 Average total strength, the sum of the three one-rep maximums, increased by 14.6% from 94.0 kg to 107.7 kg. 2 In contrast, in the advanced group the average one-rep max chest press increased by 2.7% from 44.8 kg to 46.0 kg, average one-rep max knee extension increased by 6.3% from 52.4 kg to 55.7 kg, and average one-rep max preacher curl increased by 4.9% from 24.3 kg to 25.5 kg. 2 Total strength increased 4.8% from 121.8 kg to 127.6 kg. 2 These findings go in line with other research that states that exercise benefits are most dramatic when you start a new regimen.
Similarly, body composition had more significant changes in the novice group; their body fat decreased by 3.1% from 38.7 kg to 37.5 kg and skeletal muscle mass increased 4.3% from 16.4kg to 17.1kg. 2 In contrast, in the advanced group, body fat decreased non-significantly by 0.3% from 37.3 kg to 37.2 kg, and skeletal muscles mass increased by 1% from 19.2 kg to 19.4 kg. 2 These findings suggest that resistance training decreases fat in addition to increasing muscle mass, at least when starting off the regimen.
The biomarkers painted a more varied and interesting picture. Both groups experienced favorable changes in all six biomarkers measured. This data provides further evidence that resistance exercises confer benefits beyond aesthetic, strength, and body composition. They can also lower your risk of developing cardiovascular diseases and an onslaught of other chronic conditions. Thus, the scientists concluded that “the results suggest that the RT is an effective strategy to… improve blood glucose and lipid profile of older women.” 2
Four of the five biomarkers in the metabolic profile had larger decreases in the novice group compared to the advanced group. In the novice group, triglycerides decreased an average of 12.9% from 133.7 mg/dL to 116.5 mg/dL, total cholesterol decreased an average of 1.9% from 212.2 mg/dL to 208.2 mg/dL, HDL-C increased an average of 6.7% from 53.6 mg/dL to 56.1 mg/dL, and LDL-C decreased an average of 34.0% from 132.7 mg/dL to 87.6 mg/dL. 2 In the advanced group, triglycerides decreased an average of 5.7% from 110.1 mg/dL to 103.8 mg/dL, total cholesterol changed non-significantly, HDL-C increased by 2.6% from 57.4 mg/dL to 58.9 mg/dL, and LDL-C decreased an average of 25.4% from 107.0 mg/dL to 79.8 mg/dL. 2
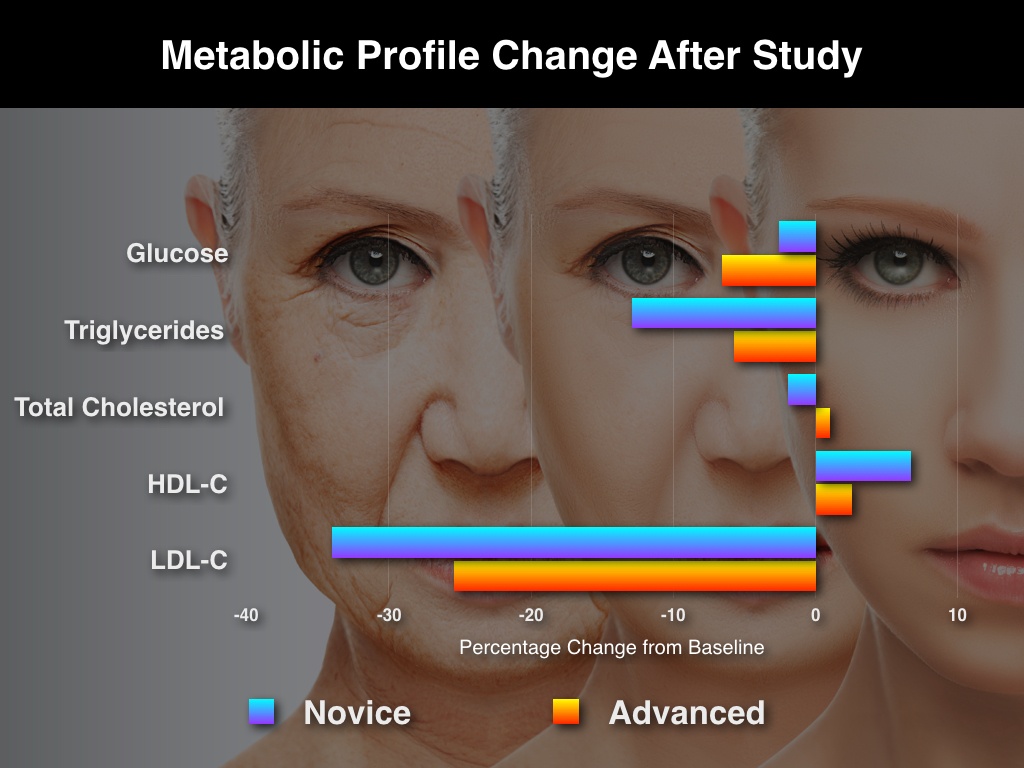
However, the experienced lifters experienced more favorable changes in glucose than the novice group. While average blood glucose concentration in the advanced group decreased by 6.6% from 99.9 mg/dL to 93.3 mg/dL, average blood glucose concentration in the novice group decreased by 2.6% from 95.8 mg/dL to 93.3 mg/dL. 2 Most surprisingly, while CRP decreased by 54.5% in the advanced group, it decreased by only 22.9% in the novice group. 2 This suggests that sticking with your resistance program is more than just for maintaining optimal health- it can further enhance it.
Summary: As expected, the study showed that weightlifting increased strength and skeletal muscles in all subjects. These changes were more pronounced in the less experienced novice group. The novice group had greater decreases in biomarkers related to cardiovascular health such as triglycerides and cholesterol. However, the advanced group had more significant changes in CRP and glucose than the novice group after the same eight-week phase of training.
Analysis: Putting the Research in Context
Some of the results from the study were expected. When you start lifting weights, you are going to get stronger and increase your muscle mass. While this study was done on older, healthy women, this has been observed in subjects of all ages in both genders.
Others were a bit more interesting. Strength training apparently optimizes biomarkers related to cardiovascular health. As previously mentioned, the novice group experienced significant decreases in triglycerides and LDL-C and a large increase in HDL-C. High levels of triglycerides and LDL-C and low levels of HDL-C are associated with increased risk of cardiovascular diseases. A lot of other literature has shown that resistance training optimizes these biomarkers in both men and women of all ages.
The most interesting finding of the study, however, was that sticking with resistance training confers unique benefits in regards to inflammation and energy regulation as shown by lower levels CRP and glucose. The advanced group had a greater average decline in CRP during the third-phase of the study when compared to the novice group. A lot of research has shown an association between decreasing body fat and lowering CRP. 16,17,18 However, it is important to emphasize that while the advanced subjects had greater decreases in CRP, they had much smaller changes in body fat compared to the novice group. Thus, the researchers emphasizes that “these findings suggest that factors other than body composition changes are responsible for CRP decreases in those with RT experience.” 2
This phenomenon could be best explained by the fact the muscle contraction produces molecules called myokines that reduce inflammation and ultimately lower levels of CRP. Because advanced strength-trainers have more muscle mass, they will produce greater levels of myokines. These findings are supported by a 2014 meta-analysis evaluating the impact of resistance training on CRP levels in elderly subjects. In these eight randomized-control studies, both moderate aerobic and resistance exercise (without overtraining) consistently contributed to a long-term decrease in CRP. Thus, the researchers concluded that “independent of losses of fat mass, exercise also increases muscle production of IL-6 which is known to reduce inflammation and increase anti-inflammatory cytokines” 19 Similarly, a study on sedentary middle-aged males showed that resistance training led to greater decreases in CRP levels than aerobic exercise. 20 Another high-quality study on athletic females noted that endurance exercise combined with strength training led to greater decreases in CRP levels than endurance exercise alone. 21
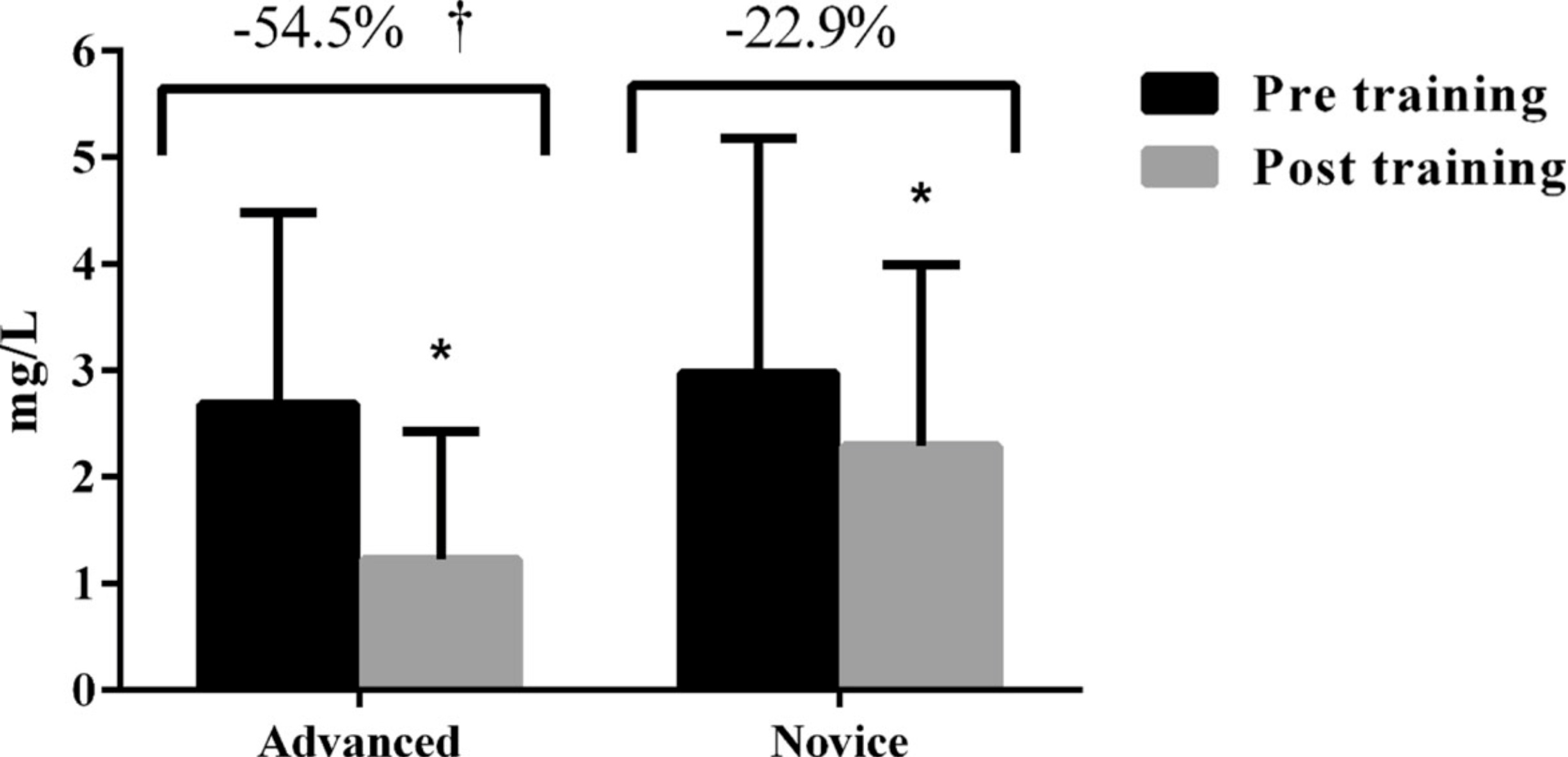
Source: S. Cyrino 2015
Additionally, glucose levels in the advanced group decreased almost three times as much compared to the novice group during the third phase of the experiment. This is explained by the fact that continued resistance training increases the sensitivity of cells to insulin, therefore decreasing blood glucose levels. 22 The researchers stated that unlike with CRP, this observation is more consistent with scientific theory and other literature. Nonetheless, it is important to note that continued resistance training can lead to greater prevention of metabolic disorders by further decreasing glucose concentrations in the blood. 2
Summary: The most interesting finding of the study was that continued resistance training leads to greater reduction in inflammation as measured by lower levels of CRP in advanced strength-trainers. Glucose levels also decrease substantially in advanced weight-lifters while novice strength-trainers experience more pronounced decreases in triglycerides and LDL-cholesterol.
Key Takeaways: What does this Study Mean to you?
What can we take away from this research study and other associated literature? Basically, regular weight training two to three times a week:
- Weight training can do a lot more than just make you stronger. It helps optimize biomarkers indicative of overall wellness such as triglycerides, LDL-cholesterol, and HDL-cholesterol in both men and women
- There may be unique benefits to sticking with a resistance training program. While changes in strength and some biomarkers taper off after you start strength-training, markers of inflammation (CRP) and energy utilization (glucose) decrease more as you continue

What impact will strength-training have on you and your biomarkers? The only way to truly know is to start, or continue, a total-body resistance training regimen and monitor the results using InsideTracker. The results of recent literature are promising, but the subjects in these studies are primarily older subjects and people can react differently to a clinical intervention such as strength-training. Will your triglyceride and LDL-C levels go from “high” to “optimal”? Will you see a prolonged decrease in glucose and CRP from a long-term adoption of kettlebells or deadlifts? If you avoid overtraining, can you see a long-term decrease in CRP from demanding regimens such as Spartan and Crossfit? A blood analysis can give you crucial information on your progress to see if you are optimizing your health and fitness. And remember to get enough rest- or your CRP levels might increase because of overtraining!
Wondering what ALL of your biomarkers mean? We've created this handy biomarker guide for reference—it's FREE & it's yours to download!

Some other blog posts we think you'll love:
- Tired of Being Tired: How I Optimized My Iron Levels
- Getting Back on Track: Laura Ingalls' InsideTracker-Fueled Journey Back to Holistic Health
- Avoiding The Crash: How Monitoring Iron Levels Can Save Your Season
- Stress Fractures: The Relationship Between Biochemistry, Nutritional Screening and Biomechanics
List of References
1. Pollock, M. L., et al. "American College of Sports Medicine Position Stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults." Med Sci Sports Exerc 30.6 (1998): 975-91.
2. Ribeiro, Alex S., et al. "Effect of resistance training on C-reactive protein, blood glucose and lipid profile in older women with differing levels of RT experience."AGE 37.6 (2015): 1-11.
3. Ridker, Paul M. "C-reactive protein—a simple test to help predict risk of heart attack and stroke." Circulation 108.12 (2003): e81-e85.
4. Azar, Rima, Robert P. Nolan, and Donna E. Stewart. "Listening to the heart-brain talk: persistent depressive symptoms are associated with hsCRP in apparently healthy individuals at high risk for coronary artery disease." European Journal of Preventive Cardiology 19.4 (2012): 857-863.
5. Fatouros, Ioannis G., et al. "Cell-free plasma DNA as a novel marker of aseptic inflammation severity related to exercise overtraining." Clinical Chemistry 52.9 (2006): 1820-1824.
6. Grundy, Scott M., et al. "Diagnosis and management of the metabolic syndrome an American Heart Association/National Heart, Lung, and Blood Institute scientific statement." Circulation 112.17 (2005): 2735-2752.
9.Miller, Michael, et al. "Triglycerides and cardiovascular disease a scientific statement from the American Heart Association." Circulation 123.20 (2011): 2292-2333.
8. Hanukoglu, Israel. "Steroidogenic enzymes: structure, function, and role in regulation of steroid hormone biosynthesis." The Journal of steroid biochemistry and molecular biology 43.8 (1992): 779-804.
9. Olson, Robert E. "Discovery of the lipoproteins, their role in fat transport and their significance as risk factors." The Journal of nutrition 128.2 (1998): 439S-443S.
10. Barter FJ, et al. Anti-inflammatory properties of HDL. Circulation Research. 2004; 95: 764-772
11. Real, J. T., et al. "Importance of HDL cholesterol levels and the total/HDL cholesterol ratio as a risk factor for coronary heart disease in molecularly defined heterozygous familial hypercholesterolaemia." European heart journal 22.6 (2001): 465-471.
12. Barter, Philip, et al. "HDL cholesterol, very low levels of LDL cholesterol, and cardiovascular events." New England Journal of Medicine 357.13 (2007): 1301-1310.
13. Germano, Giuseppe, et al. "European Guidelines on cardiovascular disease prevention in clinical practice (version 2012)." European Heart Journal 33 (2012): 1635-1701.
14. Neaton, James D., et al. "Serum cholesterol level and mortality findings for men screened in the Multiple Risk Factor Intervention Trial." Archives of internal medicine 152.7 (1992): 1490-1500.
15. Cromwell, William C., et al. "LDL particle number and risk of future cardiovascular disease in the Framingham Offspring Study—implications for LDL management." Journal of clinical lipidology 1.6 (2007): 583-592.
16. Winett, Richard A., and Ralph N. Carpinelli. "Potential health-related benefits of resistance training." Preventive medicine 33.5 (2001): 503-513.
17. Pollock, Michael L., et al. "Resistance exercise in individuals with and without cardiovascular disease benefits, rationale, safety, and prescription an advisory from the committee on exercise, rehabilitation, and prevention, council on clinical cardiology, American Heart Association." Circulation 101.7 (2000): 828-833.
18. Williams, Mark A., et al. "Resistance exercise in individuals with and without cardiovascular disease: 2007 update a scientific statement from the american heart association council on clinical cardiology and council on nutrition, physical activity, and metabolism." Circulation 116.5 (2007): 572-584.
19. Woods, Jeffrey A., et al. "Exercise, inflammation and aging." Aging and disease 3.1 (2014): 130-140.
20. Donges, Cheyne E., Rob Duffield, and Eric J. Drinkwater. "Effects of resistance or aerobic exercise training on interleukin-6, C-reactive protein, and body composition." Medicine and Science in Sports and Exercise 42.2 (2010): 304-313.
21. Daray, Laura A., et al. "Endurance and resistance training lowers C-reactive protein in young, healthy females." Applied Physiology, Nutrition, and Metabolism 36.5 (2011): 660-670.
22. Phillips, Stuart M., and Richard A. Winett. "Uncomplicated resistance training and health-related outcomes: evidence for a public health mandate." Current sports medicine reports 9.4 (2010): 208.








